Insights
J.S. Held Acquires Shechter & Everett to Expand Forensic Accounting Capabilities for Family Law Disputes in Florida
Read MoreTo err is human. We have short attention spans and get distracted easily. We have unreliable memories and forget. We have a limited ability to process information, and we overgeneralize rules-of-thumb to the wrong situations. We are biologically driven to minimize mental and physical effort. We have a wide range of abilities and disabilities. Each of us is unique in every imaginable way, and yet we are all the same in that we err.
The aftermath of error can be tragic in the field of healthcare. It is estimated that most of the serious harm and death in clinical settings is preventable [1], and some projections even distinguish medical errors as the third leading cause of death in the United States. [2] It is important to clarify, though, that not all medical errors occur because of human error per se. In reality, use errors often reflect problems with the device labeling, user interface, or other aspect of the device design. [3] Occasional human error is inevitable, but the likelihood that it occurs can be reduced through user-centered design, which is a key tenet in the field of human factors. The idea is that the designs of devices and systems should conform to the behaviors, abilities, and limitations of users—not the other way around.
As a human factors expert, it is tempting to assume that everyone recognizes the inherent benefits of user-centered design, but this is not so. Medical device companies may not see the value in human factors beyond satisfying regulatory requirements, and even those requirements may be misunderstood. [4] This disconnect likely stems from incomplete messaging by way of human factors advocates. The default argument is almost always limited to the benefits of user-centered design for altruistic outcomes such as safety and effectiveness. Although this argument is no doubt valid, it may fall short in appreciating the fact that medical device companies are businesses. In order to fulfill any purpose, the company must remain operational, and, in order to remain operational, decision-makers must consider practical outcomes rather than (or at least in addition to) altruistic ones. The messaging fails in conveying that these are not competing interests. In fact, there are a number of entirely pragmatic reasons to conclude that prioritizing human factors is simply a good business strategy.
In this article, we review the value of human factors research and user-centered design from a business perspective. After briefly clarifying these concepts, the discussion turns to the primary reasons medical device companies should care deeply about human factors, beyond safety and effectiveness.
Human factors is not so much a single discipline as it is the overlap of many, including but not limited to cognitive and developmental psychology, ergonomics, biomechanics, kinesiology, human-computer interaction, and industrial-organizational engineering. The essence of human factors research is to leverage knowledge from these disciplines to optimize interactions between humans, the tools they use, and the environments in which they use them. Does that sound like an exceedingly broad definition? It is, and that is because the qualities of user-device interactions are exceedingly complex.
For example, a device is usable if it allows users to do what they want with it easily and with minimal guidance. However, usability is an umbrella term that prompts a litany of other questions. Is the device intuitive to learn initially? How well can users return to it after a delay and recall what to do? Is the workflow efficient? How common are errors, how severe are they, and how can users recover from them? Even if a device is usable for “typical” users, it may be unusable for “atypical” users. What if the user is color blind? What if they have impaired dexterity or poor grip strength? What if they have dyslexia? Even if a device is usable and accessible, it may offer a suboptimal user experience (UX), which encompasses myriad subjective opinions, perceptions, attitudes, beliefs, and emotions. Is the device pleasant to use? Do users trust it to function as intended? Do they understand how it works and feel in control? Do they desire to use it and find that it satisfies a need? The point here is to stress that the human factors approach is holistic and extends far beyond merely verifying that users can follow a series of steps.
User-centered design is an iterative design process that is grounded in human factors. The aim is to continually assess and refine the design at the level of discrete interactions between the user and device. There are three classic principles of user-centered design: [5]
The preceding discussion implies that human factors research and user-centered design are critical for optimizing user-device interactions, and also that testing should be done early and often. However, doing so requires the allocation of finite resources. This raises an obvious question—why is it worth the investment?
Are you looking for a compelling reason to care about human factors? You have to.
The Food and Drug Administration (FDA) requires manufacturers to perform and report Human Factors Engineering and Usability Engineering (HFE/UE) testing in order to gain approval or clearance for applicable medical devices to enter the United States market. [8] The purpose is to demonstrate that the device can be used safely and effectively by the intended users, for the intended uses, and in the intended use environments. The FDA offers guidance to support the industry with submissions. With this guidance in hand, achieving HFE/UE compliance should be a simple box-checking exercise, right? Wrong.
Over 90% of first-time HFE/UE submissions to the FDA are rejected. [9] Some reasons for rejection are relatively minor and easy to avoid (such as missing or incomplete documents), but others can be disastrous at such a late stage and demand massive efforts to resolve (such as serious use-related risks that require redesigning the user interface). Regardless of the reason, resubmissions are frustrating, tedious, and can be quite costly in terms of time and money. For example, the review process can persist for months or even years, with average regulatory agency decision times between 150 and 400 days. [10] The actual and opportunity costs of initial rejections can be devastating, especially for startups and small companies with limited resources available to weather the storm of a time-to-market delay.
Other than having a finalized and user-friendly device to begin with, being part of the 10% involves fully understanding the minimum requirements. The excerpt depicted below outlines the main sections of a compliant HFE/UE report, directly from an FDA guidance document. [11] As is evidenced by such a high rejection rate, these requirements are more involved in practice than they may appear to be on paper. Therefore, medical device companies are strongly advised to enlist support from others who have prior experience with successfully navigating the submission process (including third-party consultants with relevant expertise). It only takes a single misstep for the FDA to request an inopportune resubmission.
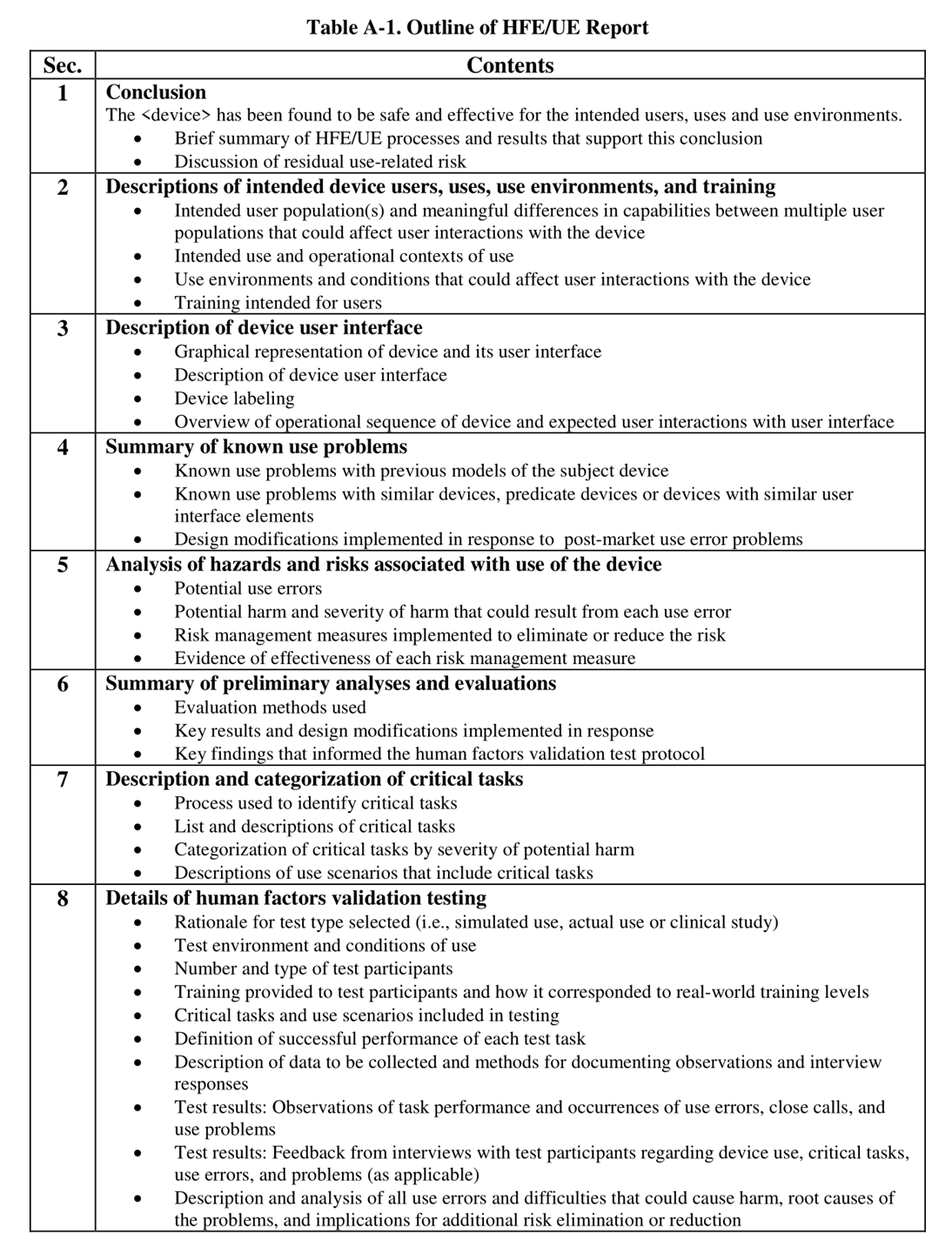
Figure 1 - Excerpt from Food and Drug Administration (2016, p. 36) guidance.
A more detailed discussion of HFE/UE regulatory requirements is beyond the scope of this article, but the validation study is worth emphasizing. It is the final definitive test to demonstrate what the manufacturer ideally already knows—namely, that the device can be used safely and effectively under realistic conditions. The main (but nonexhaustive) constraints for HFE/UE validation testing include that:
Ancillary issues related to the scope, design, execution, documentation, or reporting of the HFE/UE validation study are extremely common reasons for FDA rejection. More so than in any other aspect of the regulatory pathway, guidance from individuals who have gone through the process before (including third-party consultants who specialize in supporting regulatory submissions) is a considerable advantage. A clear understanding of what the FDA expects to see and how they expect to see it, when and how to push back on FDA reviewer feedback, and how to navigate suboptimal findings can be invaluable. A lack of this understanding contributes to the high first-time rejection rate.
Early in the design process, there are near infinite ways in which the design of a user interface can be changed, and doing so may be as simple as editing a wireframe. However, as the device lifecycle progresses, the working design gradually becomes less malleable, and changes become increasingly expensive and laborious. A change as trivial as moving the location of a button eventually requires manufacturing new prototype molds, updating the instructions for use that now specify an old location, illustrating new figures for the quick start guides that now display an outdated layout, and so on. At a certain point, the costs of making changes become so prohibitive as to be utterly impractical. The diagram depicted below is often adapted to illustrate this relationship. [13]
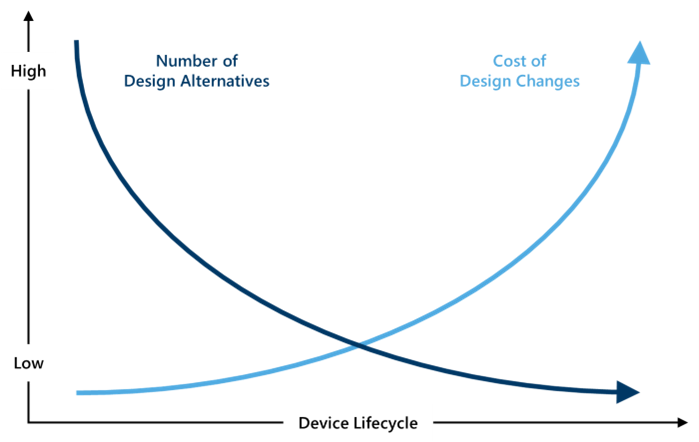
Figure 2 - Relationship between design alternatives and costs of changes throughout the device lifecycle.
Early changes are cost-effective changes, and this is a perfectly good reason to conduct human factors research early and often. In the lead up to the HFE/UE validation study, a pre-validation study following the same protocol is also prudent to verify that the device is ready for the big show. The most unwelcome finding during a validation study is not necessarily a use error—it is a use error for which there are no design controls or one which has never been seen before. No device is expected to be error-free, and the FDA fully expects there to be residual use-related risk even when best practices are followed throughout the design process. [14] Nevertheless, in the event that validation testing reveals serious use-related risks that are entirely unmitigated, the FDA will probably reject the submission and require changes to be made. It is far more economical to get ahead of the curve and probe for critical issues earlier in the development process.
The medical device industry is booming. The number of new medical devices authorized per year has increased fivefold over the past 15 years. [15] Increases in medical device spending rates have outpaced those of medical device prices, implying that the market remains fairly price competitive. [16] Interestingly, the industry also appears to be resilient to monopolization. According to census data, the vast majority of device supplies and equipment manufacturers are small-to-medium-sized with fewer than 50 employees. [17] The industry is undoubtedly a large pie, but it has many slices. This competition can be daunting, especially for young medical device companies looking to carve out a niche. The competition can be even more daunting for companies pursuing FDA clearance through the most common 510(k) pathway, which demands that similar predicate devices already exist in the market. How is product differentiation possible in such an overcrowded industry, particularly in the presence of comparable competitor devices?
The path to differentiation can be clarified by adapting the classic Kano model [18], which illustrates the effects of different product qualities on user satisfaction. Considering the regulatory requirements, every device in the market can be assumed to be reasonably safe and effective. Hence, these are must-be qualities that are simply expected to exist. Users are unlikely to appreciate or even notice if a device is slightly safer than the rest, but they will almost certainly notice and in turn abandon a device if it is uniquely unsafe. Usability and accessibility are performance qualities that can either increase or decrease satisfaction based on their execution (and relative to the bare minimum requirements). The mental workload incurred by users is an underappreciated element in this regard. Lastly, the features that contribute to the UX of a device are attractive qualities that may be unexpected and may not lead to dissatisfaction or abandonment when they are lacking but nonetheless tend to dramatically increase satisfaction when they are executed well. The diagram depicted below is often adapted to illustrate these dynamics.
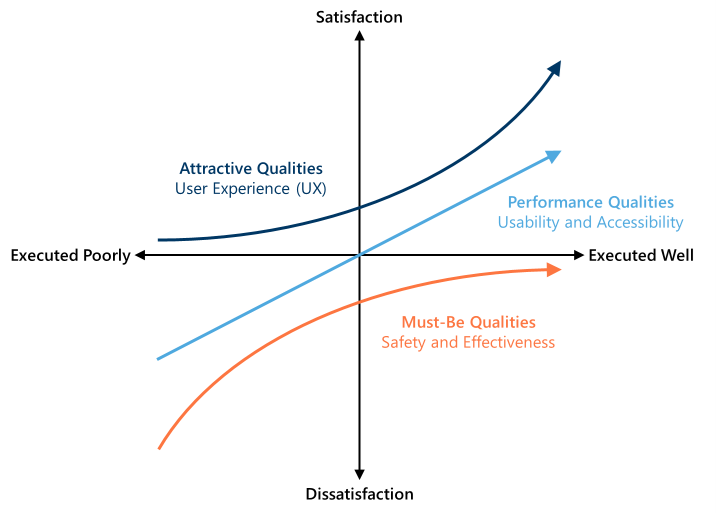
Figure 3 - Dynamics between different product qualities and user satisfaction.
When deciding among medical devices or healthcare products that are assumed to be equal in their safety, effectiveness, or other requisite qualities, UX is the deciding factor. Indeed, this view is evident in the consumer product industry, where optimizing UX has long been the secret sauce for differentiation. The medical device industry is no different in this sense. Consumers may pay a premium for gel caps over tablets—not because they are more effective, but because they are more pleasing to swallow. [19] Parents may elect to take their child to a distant hospital—not because it is more prestigious, but because their magnetic resonance imaging (MRI) machine resembles a submarine and puts their fearful child at ease during a potentially traumatic experience. [20] Insulin-dependent patients may gravitate toward nasal sprays or pricey autoinjectors with sheathed needles—not because the delivery is safer, but because those patients have an aversion to needles. [21] Thoroughly understanding the behaviors, wants, needs, and decision processes of users does not happen organically. It requires proactive effort. Methods such as user interviews, focus groups, diary studies, contextual inquiry, and other UX research approaches are critical for identifying unmet user needs and informing solutions to capture the market. It is rare for any product to satisfy a user need that the designers never knew existed.
Over the past few years, the number of medical device recalls in the United States has consistently risen, which has led some authors to call for more stringent safety and quality controls. [22] Postmarket adverse events—resulting in recalls, warning letters, warranties, lawsuits, and loss of revenue—are estimated to cost the industry between $2.5 and $5 billion per year on average. [23] This is not to mention the immeasurable negative effects that these events have on consumer trust and brand perception. The reality is that, whether or not the FDA requires a study to demonstrate safety and effectiveness for a given device, it is unrealistic that any single study could uncover every possible (exotic) way in which users will use, misuse, or become harmed by a device in the real world. This is partly why diligent postmarket surveillance, as required by the FDA, is so important, in addition to formative testing and development performed to the extent feasible. It is only through extensive testing and retesting that medical device companies can more fully appreciate the universe of potential misuses in practice and decide whether further action is warranted. Adopting a habit of routine research on usability, accessibility, safety, and effectiveness is like obtaining an insurance policy. Iterative research further establishes a documented history of proactive due diligence, which is sure to become handy in the worst-case scenario of litigation.
As the adage goes, it takes money to make money, and it most certainly takes money to launch a startup or small company in the medical device space. Hundreds of billions of dollars are invested annually in medical and health research and development, most of which is from investors in the private sector. [24] Justifying that a company is worth venture capital can be an uphill battle. Savvy investors want tangible evidence that a company understands its market segment, has identified a need, and has created a device to satisfy that need better than competitors. [25] Especially if a device would be more expensive than alternative options in the market, actual data from user research may be essential to justify the expectation that users will abandon their current device and adopt another. Establishing a robust human factors research program also demonstrates to investors that a company values evidence-based decisions, prioritizes the needs of the users, strives for improvement, and fully understands the regulatory requirements. Moreover, research inevitably breeds innovation, and groundbreaking companies quickly become targets for mutually beneficial acquisitions or mergers with larger conglomerates.
The human factors research toolbox is diverse, and mighty oaks grow from little acorns. Sure, deeply informative insights into user-device interactions can be gleaned through state-of-the-art research methods such as motion capture and eye tracking. [26] However, many companies simply have neither the capital to invest in these complex approaches nor a complete understanding of what insights those techniques can offer.
Fortunately, there are many quick, easy, and frugal strategies that can maximize returns on rather small engagements. Are you concerned about your first FDA submission and worry that something is missing? A regulatory gap analysis can be commissioned to thoroughly audit your submission package against applicable regulatory requirements and identify and resolve any gaps that may exist. Do you want to better understand your target user population or opportunities for improvement in your market segment? A small-scale or remote study using online crowdsourcing services, a literature review, or an analysis of postmarket surveillance databases can help inform that understanding. Do you want high-level design feedback without incurring the costs of laboratory rental, participant recruitment, and in-person testing? A heuristic evaluation is one of the most fruitful alternatives, wherein a bona fide human factors expert systematically evaluates the quality of the user interface against established design principles (the heuristics) to uncover any prospective issues. [27] The most suitable research approach depends on the questions at hand, but the value of research itself does not hinge on complexity or cost.
It is prudent for medical device companies to prioritize human factors because doing so offers a profound and measurable benefit to the safety and welfare of end users. This is truly a compelling argument, but it is also an incomplete one. Executives are often confronted with tough decisions like how to wisely allocate time, money, and other finite resources. For better or for worse, there is a balance to be struck between what is best for the user and what is best for the company. The goal of this article is to expand and defend the proposal that prioritizing human factors is both good for the user and good for business. As it turns out, the rationale remains strong even when only considering outcomes such as time-to-market, design costs, product differentiation, corporate risk, and venture capital. This is especially true when considering that, with the right expertise, even a decidedly small research engagement can deliver an enormous return on investment. Human factors is more than a box to check, and it is important to acknowledge the value in involving human factors experts when and where appropriate. Insight from human factors research can be a powerful catalyst for innovative design and an underestimated driver of business growth.
We would like to thank our colleague Joseph Pauszek, Ph.D. for providing insight and expertise that greatly assisted this research.
Joseph Pauszek, Ph.D. is a Managing Scientist of Human Factors at J.S. Held. He has over a decade of experience conducting research in academia and industry on various topics, including visual attention and distraction, cognitive workload and mental effort, stress, working memory, rational decision-making, perception, information processing, user experience, safety, and effectiveness of both consumer products and medical devices. Dr. Pauszek has also cultivated specialized experience in healthcare research, and in the evaluation of medical devices that range in complexity from autoinjectors to robotic surgery systems. This proficiency spans all stages of the medical device lifecycle, from early-stage formative research to formal human factors engineering and usability engineering (HFE/UE) submissions to satisfy regulatory requirements. Dr. Pauszek operates out of J.S. Held’s state-of-the-art scientific User Research Labs (URL) at the Phoenix, AZ, location.
Dr. Pauszek can be reached at [email protected] or +1 480 914 9228.
[1] Panagioti, M., Khan, K., Keers, R.N., Abuzour, A., Phipps, D., Kontopantelis, E., Bower, P., Campbell, S., Haneef, R., Avery, A.J., & Ashcroft, D.M. (2019). Prevalence, severity, and nature of preventable patient harm across medical care settings: Systematic review and meta-analysis. BMJ, 366, i4185.
[2] Makary, M.A., & Daniel, M. (2016). Medical error – The third leading cause of death in the US. BMJ, 353, i2139.
[3] Food and Drug Administration (2016). Medical device reporting for manufacturers. https://www.fda.gov/media/86420/download (accessed 04/01/2025).
[4] Money, A.G., Barnett, J., Kuljis, J., Craven, M.P., Martin, J.L., & Young, T. (2011). The role of the user within the medical device design and development process: Medical device manufacturers’ perspectives. BMC Medical Informatics and Decision Making, 11(15), 1-12.
[5] Gould, J.S., & Lewis, C. (1985). Designing for usability: Key principles and what designers think. Communications of the ACM, 28(3), 300-311.
[6] Food and Drug Administration (2016). Applying human factors and usability engineering to medical devices. https://www.fda.gov/media/80481/download (accessed: 02/25/2025).
[7] In practice, there is often a need to balance representativeness with logistical constraints. Research conducted with lower-fidelity wireframes or mockups can still be informative and may be warranted in some cases, such as when the curation of high-fidelity or truly representative prototypes is exceedingly costly or otherwise infeasible.
[8] It is worth acknowledging that some exceptions and exemptions exist, although they are exceedingly rare.
[9] Rojas, K.M., Sharareh, N., Cosier, L., & Santos, D.L. (2019). Considering the dynamics of FDA human factors validation requirement: Implications of failure and need to ensure project success – A conceptual framework. In Proceedings of the International Symposium on Human Factors and Ergonomics in Health Care (pp. 234-247).
[10] Aboy, M., Crespo, C., & Stern, A. (2024). Beyond the 510(k): The regulation of novel moderate-risk medical devices, intellectual property considerations, and innovation incentives in the FDA’s De Novo pathway. NPJ Digital Medicine, 7(1), 29.
[11] Food and Drug Administration (2016). Applying human factors and usability engineering to medical devices. https://www.fda.gov/media/80481/download (accessed: 02/25/2025).
[12] As noted previously, “use errors” occur during use but may not necessarily be attributable to the “user” per se.
[13] Raj, K.P., & Veeramani, G. (2018). Marketing based decision making process in engineering design. International Journal of Engineering & Technology, 7(4.36), 854-858.
[14] Food and Drug Administration (2016). Applying human factors and usability engineering to medical devices. https://www.fda.gov/media/80481/download (accessed: 02/25/2025).
[15] Center for Devices and Radiological Health (2024). 2024 CDRH innovation report. https://www.fda.gov/media/177865/download?attachment (accessed: 02/25/2025).
[16] Donahoe, G.F. (2021). Estimates of medical device spending in the United States. Advanced Medical Technology Association. https://www.advamed.org/wp-content/uploads/2021/12/Estimates-Medical-Device-Spending-United-States-Report-2021.pdf (accessed 02/25/2025).
[17] U.S. Census Bureau (2023). CB2100CBP: NAICS 3391: medical equipment and supplies manufacturing: 2021. https://data.census.gov/table/CBP2021.CB2100CBP?g=010XX00US&n=3391 (accessed 02/25/2025).
[18] Kano, N., Seraku, K., Takahashi, F., & Tsuji, S. (1984). Attractive quality and must-be quality. Journal of the Japanese Society for Quality Control, 14(2), 147-156.
[19] Jones, W.J., & Francis, J.J. (2000). Softgels: Consumer perceptions and market impact relative to other oral dosage forms. Advances in Therapy, 17(5), 213-221.
[20] Good News Network (2020). From terrifying to terrific: Man redesigns MRI machine to delight children instead of scare them. https://www.goodnewsnetwork.org/terrifying-terrific-man-redesigns-medical-machine-delight-children-instead-scare/ (accessed 02/25/2025).
[21] Bajpai, S.K., Cambron-Mellott, M.J., Peck, E., Poon, J.L., Wang, Q., Mitchell, B.D., Barbrowicz, J., Child, C.J., Raibulet, N.K., & Beusterien, K. (2019). Perceptions about glucagon delivery devices for severe hypoglycemia: Qualitative research with patients, caregivers, and acquaintances. Clinical Therapeutics, 41(10), 2073-2089.
[22] Aaliya Parvin, M.J., Sudheer Kumar, T., & Kamaraj, R. (2024). A comprehensive analysis of Class I medical device recalls: Unveiling patterns, causes and global impacts. Cureus, 16(8), e67542.
[23] Fuhr, T., George, K., & Pai, J. (2013). The business case for medical device quality [white paper]. McKinsey.
[24] Research!America (2022). U.S. investments in medical and health research and development: 2016 – 2020. https://www.researchamerica.org/wp-content/uploads/2022/07/ResearchAmerica-Investment-Report.Final_.January-2022.pdf (accessed: 02/25/2025).
[25] Mas, J.P., & Hsueh, B. (2017). An investor perspective on forming and funding your medical device start-up. Techniques in Vascular and Interventional Radiology, 20(2), 101-108.
[26] Pauszek, J.R. (2023). An introduction to eye tracking in human factors healthcare research and medical device testing. Human Factors in Healthcare, 3, 100031.
[27] Zhang, J., Johnson, T.R., Patel, V.L., Paige, D.L., & Kubose, T. (2003). Using usability heuristics to evaluate patient safety of medical devices. Journal of Biomedical Informatics, 36(1-2), 23-30.
A Q&A article about the role human factors and user experience play in medical and patient safety and in medical product design,...
While telemedicine visits and digital health records have brought about significant improvements in healthcare accessibility and efficiency, they also present unique challenges in the context of casualty claims and injury assessment. Our practice has seen...